
Published on Sep 17, 2025
Daily Current Affairs
Current Affairs 17 September 2025
Content
- Top court asks who will decide that a religious conversion is ‘deceitful’
- Making health care safe for every Indian
- Unseen labour, exploitation: the hidden human cost of Artificial Intelligence
- India Targets Record 119 MT Wheat Output in 2025-26
- Heavy Rains in the Himalayas: Interplay of Topography, Climate Change, and Rising Disaster Risks
Top court asks who will decide that a religious conversion is ‘deceitful’
Basics
- Issue: A petition before the Supreme Court seeks a ban on “deceitful” religious conversions and questions the constitutionality of State-level anti-conversion laws.
- Constitutional Context:
- Article 25: Provides freedom of conscience and right to profess, practice, and propagate religion, subject to public order, morality, and health.
- Supreme Court in Rev. Stanislaus vs State of MP (1977) upheld States’ power to regulate conversion by force, fraud, or inducement.
- State Laws: Around 10 States (UP, MP, Gujarat, Himachal, Uttarakhand, Karnataka, Haryana, Jharkhand, Chhattisgarh, Rajasthan) have enacted Freedom of Religion Acts, often termed “anti-conversion laws.”
- Recent Hearing (Sept 2025):
- Chief Justice B.R. Gavai asked who determines if a conversion is “deceitful.”
- Petitioners argue laws are restrictive; respondents defend their necessity.
- Court will reconsider the matter after six weeks.
Relevance:
- GS-II (Polity & Governance):
- Fundamental Rights (Article 25 – freedom of religion; Articles 14, 19, 21 – equality, liberty, life).
- Judicial review of State legislation (SC role in constitutional validity).
- Federalism: Centre vs State competence in religious matters.
- GS-I (Society):
- Inter-faith relations, social harmony, religious practices.
- GS-II (Governance):
- Criminal justice reforms (burden of proof, third-party complaints).
Overview
Constitutional and Legal Dimensions
- Right to Freedom of Conscience: Protected under Article 25; scope of “propagation” does not necessarily extend to conversion.
- State Regulation: Laws seek to prevent conversions through coercion, fraud, or inducement.
- Judicial Role: SC has clarified its role is to test constitutionality, not legislate.
- Burden of Proof: Some State laws place it on the individual converting, raising constitutional questions.
Federalism
- Religion-related matters fall under the Concurrent List. States have legislated individually, sometimes using other States’ laws as models.
- Debate exists over whether a uniform central framework or diverse State laws are more appropriate.
Individual Rights and Society
- Marriage and Conversion: Many laws scrutinize inter-faith marriages linked to conversion.
- Right to Choice: Questions arise over balancing personal autonomy with State interest in regulating conversions.
- Chilling Effect: Concerns raised that ordinary religious practices could be subjected to suspicion.
Criminal Justice and Governance
- Punishment Provisions: Some Acts provide for stringent penalties, including extended imprisonment.
- Third-Party Complaints: Provisions allowing unrelated individuals to initiate proceedings create scope for wide application.
- Implementation: Conviction rates remain limited; many cases end in prolonged litigation.
Political and Social Dimensions
- Legislative Intent: Governments argue laws are preventive in nature, safeguarding vulnerable groups from coercion.
- Social Context: Critics argue laws may impact interfaith relationships and minority communities.
- Polarization Risk: Debate around conversions often intersects with political and electoral narratives.
Judicial Outlook
- Pending Issues: SC will examine if provisions violate Articles 14, 19, 21, and 25.
- Possible Judicial Outcomes:
- Striking down specific provisions (burden of proof, third-party locus).
- Upholding core objectives of preventing forcible conversion.
- Issuing guidelines for uniform application.
Making health care safe for every Indian
Basics
- Event: World Patient Safety Day observed annually on September 17, declared by WHO in 2019.
- Theme 2025: Focus on safe care for every newborn and every child (WHO campaign).
- Global Context:
- WHO estimates: 1 in 10 patients harmed during hospitalization.
- 4 in 10 patients harmed in primary/ambulatory care, with 80% of harm preventable (WHO, 2023 fact sheet).
- Indian Context:
- Disease burden shifting to chronic conditions (cancer, diabetes, CVD, mental health).
- Complexity in acute care (multi-speciality coordination) increases risk of patient harm.
Relevance:
- GS-II (Governance, Social Justice):
- Right to Health (Directive Principles, judicial debates).
- Public health institutions, policies, and regulation.
- Role of civil society and CSR in health awareness.
- GS-III (Science & Technology):
- Use of AI, EHRs, digital tools in patient safety.
- GS-II (International):
- WHO’s role, India’s commitments in global health governance.
Dimensions of Patient Harm
- Clinical Causes:
- Hospital-acquired infections, unsafe injections, transfusion errors.
- Adverse drug reactions, inappropriate medication combinations.
- Delayed diagnoses, preventable surgical errors, patient falls.
- Systemic Causes:
- Overburdened staff (low doctor-patient ratio, long shifts, attrition).
- Weak quality monitoring and low NABH accreditation (<5% of hospitals).
- Limited patient awareness, passive role in care decisions.
India’s Initiatives
- Policy & Frameworks:
- National Patient Safety Implementation Framework (2018–25) – roadmap for embedding safety in clinical programs, event reporting, capacity-building.
- NABH (National Accreditation Board for Hospitals & Healthcare Providers) – standards on infection control, patient rights, medication safety.
- Institutions & Networks:
- Society of Pharmacovigilance, India – ADR (adverse drug reaction) monitoring.
- Patients for Patient Safety Foundation (PFPSF) – awareness to 14 lakh households weekly, supporting 1,100 hospitals and 52,000 professionals.
- Patient Safety & Access Initiative – focuses on medical devices regulation.
- Civil Society & Technology:
- CSR-funded campaigns, workplace health programs, safety tech (e-prescriptions, interaction alerts).
- WHO Global Patient Safety Action Plan promotes Patient Advisory Councils (PACs) – patient representation in hospital governance.
Gaps & Challenges
- Accreditation: Out of 70,000+ hospitals in India (NHP 2023), fewer than 5% NABH-accredited.
- Awareness: Low patient literacy; hesitancy in questioning doctors.
- Implementation Gap: Policy exists but enforcement and monitoring remain weak.
- Resource Constraints: Public hospitals face overload; private sector highly fragmented.
Overview
- Polity/Governance: Patient safety ties into Right to Health debates; requires stronger regulation and accountability.
- Social: Safety lapses disproportionately affect vulnerable groups – poor, elderly, children, women in maternity care.
- Economic: Unsafe care increases out-of-pocket expenditure; WHO estimates adverse events cost trillions globally.
- Technology: AI-driven prescription checks, EHRs, digital ADR reporting can reduce risks.
- International: WHO benchmarks provide templates; India’s progress modest compared to high-income countries with strong PACs and reporting culture.
Way Forward
- Renew Patient Safety Framework (post-2025) with measurable targets.
- Strengthen NABH/NQAS accreditation coverage, link to insurance empanelment.
- Institutionalize Patient Advisory Councils in Indian hospitals.
- Integrate patient safety modules in MBBS, nursing curricula.
- Create national patient safety registry for transparent reporting of adverse events.
- Expand public participation: digital health literacy campaigns, family-based safety checklists.
Unseen labour, exploitation: the hidden human cost of Artificial Intelligence
Basics – Context of the News
- Automated Economy: Refers to increasing reliance on Artificial Intelligence (AI) and Machine Learning (ML) systems to perform tasks once handled by humans.
- Core Issue: While AI is seen as “self-learning” and autonomous, it is fundamentally dependent on invisible human labour—especially data annotators, moderators, and gig workers.
- Why It Matters:
- Challenges the myth of AI being “self-sufficient.”
- Raises ethical concerns on exploitation of low-paid workers in the Global South.
- Brings labour rights and digital economy regulations into the AI governance debate.
Relevance:
- GS-III (Economy, Science & Technology):
- Future of work, gig economy, labour market disruptions.
- AI, ML, and automation ethics.
- GS-II (Polity & Governance):
- Labour rights, regulation of digital platforms, global supply chains.
- GS-I (Society):
- Social impact of digital labour exploitation in developing countries.
Human Involvement in AI Development
- Data Annotation:
- Essential for training AI models—labelling text, images, video, and audio.
- Example:
- LLMs (ChatGPT, Gemini) learn meaning from labelled datasets.
- Self-driving cars need human-labelled data to distinguish pedestrians vs. traffic signs.
- Training Process of LLMs:
- Self-supervised learning → machine consumes raw internet data.
- Supervised learning → annotators refine the dataset.
- Reinforcement learning → humans provide feedback on AI responses.
- Specialised vs. Non-specialised Tasks:
- Some require domain expertise (e.g., medical scans, legal texts).
- Many companies hire non-experts to cut costs → leads to errors in outputs.
- Invisible Labour in “Automated” Features:
- Content moderation on social media → done by humans reviewing graphic/violent material.
- Voice and video AI → trained on performances by actors, including children.
Ghost Work – Definition
- Ghost work refers to the invisible human labour that powers supposedly “automated” digital technologies such as Artificial Intelligence (AI), Machine Learning (ML), and online platforms.
- It includes microtasks like data annotation, content moderation, labeling images/videos/text, training AI models, or cleaning datasets, often outsourced to low-paid workers in developing countries.
- The term highlights how these workers remain uncredited, underpaid, and hidden behind the façade of automation, even though their labour is indispensable to AI systems.
Nature of Exploitation
- Geography of Ghost Work: Primarily outsourced to Kenya, India, Pakistan, Philippines, China.
- Wages and Conditions:
- Reported pay: <$2/hour for 8+ hours.
- Exposure to disturbing content → PTSD, depression, anxiety.
- Tight deadlines, surveillance, microtask-based pay.
- Labour Rights Violations:
- Companies circumvent local labour laws by outsourcing through intermediaries.
- Lack of transparency: workers often don’t know which Big Tech firm they are serving.
- Union busting and dismissal of workers raising concerns.
Larger Structural Concerns
- AI’s “Dependence Myth”: Automation narrative hides human labour inputs.
- Global Inequality: Wealth and value captured in Silicon Valley, while labour exploitation occurs in the Global South.
- Informalisation of Digital Labour: Microtasking, subcontracting, gig-work fragmentation → workers have no bargaining power.
- Ethical & Social Costs:
- Mental health deterioration of moderators.
- Risk of bias/errors in AI outputs due to underqualified annotators.
- Potential exploitation of children in data collection.
Policy and Regulatory Implications
- Transparency in AI Supply Chains: Companies must disclose labour networks behind AI models.
- Fair Wages and Labour Rights: Align digital work with ILO standards (decent work, safe conditions, collective bargaining).
- Global Governance of AI Labour:
- UN/ILO frameworks for digital gig work.
- Regulation of cross-border outsourcing and labour practices.
- National-Level Actions:
- Countries like India/Kenya/Philippines need to update labour laws for gig/digital workers.
- Formalisation of data annotation industry with minimum wage guarantees.
- AI Governance Debate Expansion: Current focus is on AI ethics, privacy, bias → must include labour justice.
Overview
- Polity: Raises questions of labour rights, regulation of Big Tech, role of unions.
- Economy: Exploitation lowers wages globally, undermines sustainable digital economy.
- Society: Hidden suffering of moderators and annotators shapes the “clean” digital experience of billions.
- Ethics: Transparency vs. corporate secrecy in AI supply chains.
- International Relations: North-South divide in AI’s economic benefits vs. labour burdens.
Way Forward
- Recognise “ghost workers” as integral to AI development.
- Establish global labour standards for AI-linked work.
- Strengthen worker protections: fair pay, mental health support, right to unionise.
- Push for AI supply chain audits just like environmental/ESG audits.
- Shift narrative from “AI is replacing humans” to “AI is built on human labour”.
India Targets Record 119 MT Wheat Output in 2025-26
Basics – Context of the News
- Background:
- India achieved an all-time high wheat production of 117.51 million tonnes in Rabi 2024–25.
- For Rabi 2025–26, the Union Agriculture Ministry has set a higher target: 119 million tonnes.
- Significance of Wheat:
- Wheat is India’s second-largest foodgrain crop after rice.
- It is the main Rabi crop, covering over 30 million hectares.
- Vital for food security under NFSA and PMGKAY (subsidised grains to ~81 crore people).
- Overall Foodgrain Target:
- Govt has set 171.14 million tonnes for Rabi 2025–26.
- Wheat is the dominant share, followed by pulses, coarse cereals, and oilseeds.
Relevance:
- GS-III (Economy, Agriculture):
- Food security, agricultural productivity, MSP and procurement.
- Crop diversification (pulses, oilseeds, millets).
- Climate-smart agriculture and input management.
- GS-II (Governance):
- Role of policies, schemes (e.g., Viksit Krishi Sankalp Abhiyan).
- GS-I (Geography):
- Cropping patterns, agro-climatic zones.
Production Targets for 2025–26 (in mn tonnes)
- Wheat → 119
- Maize → 14.5
- Total Coarse Cereals → 16.55
- Total Shri Anna (millets) → 3.17
- Gram → 11.8
- Total Pulses → 16.57
- Total Foodgrains → 171.14
- Groundnut → 0.74
- Rapeseed & Mustard → 13.9
Key Drivers & Challenges
- Favourable Factors:
- Higher seed availability: 25 million metric tonnes of seeds already stockpiled (vs requirement of ~22.9 MT).
- Expected good rainfall in several parts of India → improves soil moisture.
- Government push for balanced fertiliser supply (coordination with Ministry of Chemicals & Fertilisers).
- Launch of Viksit Krishi Sankalp Abhiyan from Oct 3 → massive outreach to farmers for awareness, technology adoption.
- Challenges/Risks:
- Climate variability: untimely rains, heat waves during March (grain filling stage).
- Rising input costs (fertilisers, diesel).
- Regional disparities in productivity (Punjab/Haryana high, eastern India lagging).
- Storage and MSP procurement bottlenecks in bumper production years.
Broader Agricultural Strategy Reflected
- Shift Beyond Wheat & Rice:
- Push for pulses and oilseeds (reduce import dependence: ~60% edible oil imported, ~20% pulses imported).
- Special focus on millets (Shri Anna) → nutrition security + climate resilience.
- Per-Hectare Productivity:
- Chouhan highlighted need for yield enhancement, not just acreage expansion.
- Crop-wise reviews, large-scale farmer meetings, and technology dissemination planned.
- Food Security + Export Angle:
- High output sustains NFSA and buffer stocks.
- Surpluses may open export opportunities, though govt often restricts wheat exports for domestic price stability.
Economic & Policy Implications
- For Farmers:
- Assured procurement of wheat at MSP (₹2275/quintal in 2025–26).
- Possible rise in incomes if productivity improves without proportional input cost rise.
- For Economy:
- Higher wheat output → helps curb food inflation.
- Reduces import dependence (especially in pulses & oils if strategy succeeds).
- For Government:
- Balancing act between procurement, storage, and subsidy costs.
- Must ensure timely fertiliser/seed availability and irrigation support.
Overview
- Polity/Governance: Strengthens govt’s food security narrative; supports welfare schemes.
- Economy: Contributes to agricultural GDP, inflation management, rural employment.
- Environment: Risk of over-dependence on wheat-paddy cycle (soil degradation, groundwater depletion). Need crop diversification.
- Technology: Precision farming, new HYVs, climate-resilient varieties critical for sustaining growth.
- International Relations: India could influence global wheat markets if production exceeds domestic demand.
Way Forward
- Focus on climate-smart agriculture (heat/drought-resistant wheat varieties).
- Incentivise crop diversification into pulses/oilseeds to reduce import bills.
- Invest in post-harvest infrastructure (storage, cold chains, logistics).
- Encourage farm mechanisation and digital extension services.
- Link wheat strategy to broader goals of Doubling Farmers’ Income & Viksit Bharat 2047.
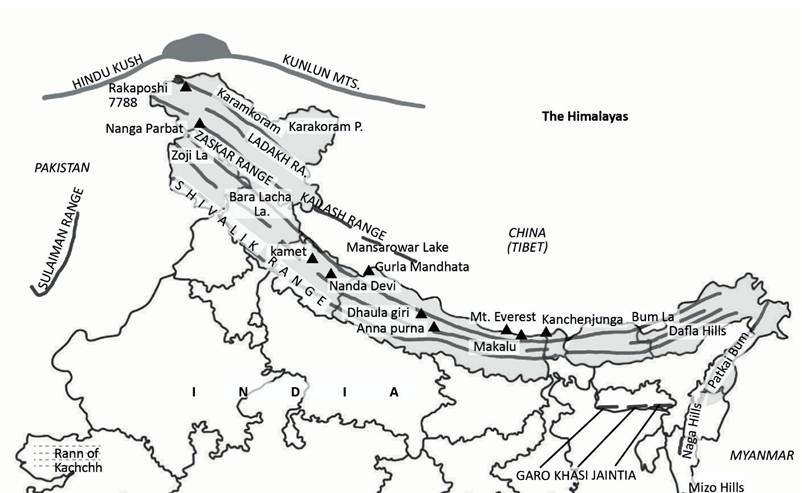
Heavy Rains in the Himalayas: Interplay of Topography, Climate Change, and Rising Disaster Risks
Basics – Context of the News
- Event: Uttarakhand, Himachal Pradesh, and other Himalayan states have witnessed extreme rainfall, landslides, and flash floods in recent weeks.
- Impact:
- At least 15 deaths in the last few days.
- Multiple landslides, blocked roads, swollen rivers, and destruction of property.
- Pattern:
- Monsoon activity intensified in northwestern India.
- Region received 34% surplus rainfall in August 2025.
- Some districts received rainfall equivalent to an entire year’s quota in just 24–48 hours.
Relevance:
- GS-I (Geography):
- Monsoon variability, orographic rainfall, Himalayan topography.
- Disaster-prone areas (cloudbursts, landslides, flash floods).
- GS-III (Environment, Disaster Management):
- Climate change impacts, glacial melt, NDMA role.
- Vulnerability mapping and risk reduction strategies.
Why do hilly regions receive more rainfall?
- Topography effect:
- Hills force moisture-laden winds to rise, cooling them and causing rainfall (orographic effect).
- Sequential rain-bearing systems:
- Low-pressure systems from the Bay of Bengal travel northwards, increasing rainfall in the Himalayas.
- Seasonal behaviour:
- Northwest India often gets late-season (August–September) monsoon surges.
Data Highlights (Rainfall Departures)
- All-India Rainfall Departure (Aug 14–Sep 10): consistently above normal.
- Northwest India Rainfall:
- Aug 21–27: +132%
- Aug 28–Sep 3: +182%
- Sep 4–10: +57%
- Cumulative Rainfall (till Sep 15, mm):
- Uttarakhand: 1192 mm (+134%)
- Himachal Pradesh: 702 mm (+22%)
- J&K: 611 mm (+57%)
- Ladakh: 280 mm (+33%)
- Punjab/Haryana/Rajasthan: above/below normal but not as extreme as hill states.
Why are hilly regions more vulnerable?
- Steep slopes + fragile geology → high risk of landslides.
- Rivers/streams descend rapidly → cause flash floods.
- Narrow valleys funnel water and debris → more damage.
- Infrastructure exposure: roads, bridges, houses often located close to rivers and slopes.
- Examples: Udhampur (J&K) 630 mm rain in 24 hours; Leh–Ladakh 59 mm in 48 hours (highest since records began).
Role of Climate Change
- Warming atmosphere → holds more moisture, increases intensity of downpours.
- Changing monsoon patterns → longer dry spells + short bursts of extreme rainfall.
- Rising global temperatures → accelerates melting of Himalayan glaciers and snow, adding to flash floods.
- Extreme weather events becoming more frequent:
- Sudden cloudbursts.
- Intensification of western disturbances.
- Increased variability in rainfall distribution.
Disaster Linkages
- Not all heavy rains = disasters, but in Himalayas:
- Weak slopes + construction + deforestation magnify risks.
- Cloudbursts + extreme rainfall → landslides + flash floods.
- Example: Mandi, Kullu, Dharali, Tharali saw severe damage to homes, bridges, and crops.
- Human factor: Unregulated construction, road widening, and riverbank encroachments worsen vulnerability.
Overview
- Polity/Governance: State disaster preparedness, early warning systems, NDMA policies.
- Economy: Damage to roads, hydropower projects, tourism industry, agriculture.
- Society: Loss of lives, displacement, trauma in vulnerable hill communities.
- Environment: Deforestation, slope destabilisation, glacial retreat exacerbate risks.
- Technology: Need for better forecasting, Doppler radars, satellite monitoring.
Way Forward
- Strengthen early warning systems + last-mile connectivity in Himalayan states.
- Enforce scientific land use planning (ban construction in eco-sensitive zones).
- Promote climate-resilient infrastructure: slope stabilisation, drainage systems, safe housing.
- Invest in watershed management (afforestation, river restoration).
- Integrate climate change adaptation into state disaster management plans.
- Regional cooperation for Himalayan ecosystem sustainability (since many rivers are transboundary).